
If your skin suddenly feels like tissue paper, dry, thin, reactive to everything, you’re not imagining it. This isn’t about needing a better moisturiser. It’s your skin barrier collapsing in real time as estrogen drops.
Menopause doesn’t just bring hot flashes and mood changes. It triggers a structural breakdown in your skin that most dermatologists barely mention. Collagen production falls by up to 30% in the first five years after your last period. Ceramide synthesis slows. The lipid barrier that kept water in and irritants out? It thins and fractures.
And if you’re living in a hard water climate, the Gulf, Arizona, parts of Australia, the environmental assault compounds the hormonal damage. Mineral-laden water strips what little barrier function you have left. Your skin can’t recover between washes. The dryness becomes chronic. This article contains affiliate links. See our affiliate disclosure for details.
Here’s what’s actually happening to your skin during menopause, why the usual advice fails, and what works when your barrier is in crisis. Medically reviewed by Dr. Layla Hassan, Trichologist.
Key Takeaways
• Estrogen decline during menopause reduces collagen production by up to 30% in the first five years, causing skin thinning and increased fragility
• Ceramide synthesis slows significantly after menopause, weakening the lipid barrier and increasing trans-epidermal water loss (TEWL)
• Hard water minerals (calcium, magnesium) compound hormonal skin damage by stripping lipids and depositing on the already-compromised barrier
• Barrier-repair ingredients, ceramides, cholesterol, fatty acids, are more critical than anti-aging actives during perimenopause and menopause
• Gentle cleansing with chelating formulas prevents mineral buildup that worsens barrier dysfunction in hard water environments
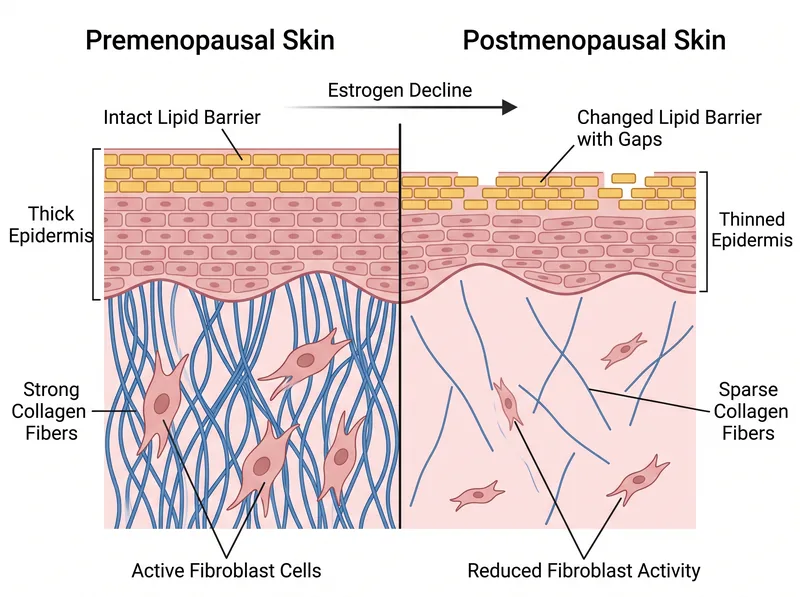 How estrogen decline affects skin structure: collagen production drops, ceramide synthesis slows, and the lipid barrier thins.
How estrogen decline affects skin structure: collagen production drops, ceramide synthesis slows, and the lipid barrier thins.
What Estrogen Actually Does for Your Skin (And What Happens When It’s Gone)
Estrogen is the master regulator of skin structure. It stimulates fibroblasts, the cells that produce collagen and elastin. It promotes hyaluronic acid synthesis, which holds water in the dermis. It regulates sebum production, keeping skin supple. And it drives ceramide production in the epidermis, maintaining the lipid barrier that prevents water loss.
When estrogen levels drop during perimenopause and menopause, all of these processes slow or stop. Research published in the American Journal of Clinical Dermatology shows that skin collagen content decreases by approximately 30% in the first five years after menopause, with a continued decline of about 2% per year thereafter.
The visible result: skin that suddenly looks and feels thinner. Fine lines deepen. The skin loses its bounce. It bruises more easily. And it becomes dramatically more sensitive to environmental stressors, including the mineral content of your water.
But the invisible damage is worse. The lipid barrier, the brick-and-mortar structure of ceramides, cholesterol, and fatty acids that seals the outermost layer of skin, begins to deteriorate. Gaps form. Water escapes. Irritants penetrate. Trans-epidermal water loss (TEWL) increases, and your skin can’t hold moisture no matter how much you apply.
The Lipid Barrier Collapse: Why Moisturiser Suddenly Stops Working
You’ve probably noticed that the moisturiser that worked for years now feels useless. It sits on the surface. Your skin drinks it and feels dry again within an hour. That’s not the product failing, it’s your barrier.
The skin’s lipid barrier is made of three key components in a specific ratio: ceramides (about 50%), cholesterol (25%), and free fatty acids (15%). This precise mixture creates a waterproof seal. When estrogen drops, ceramide synthesis slows dramatically. The ratio shifts. The seal breaks.
A study in the Journal of Investigative Dermatology found that postmenopausal women have significantly lower ceramide levels in the stratum corneum compared to premenopausal women, correlating directly with increased TEWL and barrier dysfunction.
Standard moisturisers, even rich ones, can’t fix this. They’re designed to add water or occlude the surface. But if the underlying lipid structure is fractured, water evaporates faster than you can replace it. You need barrier repair, not just hydration.
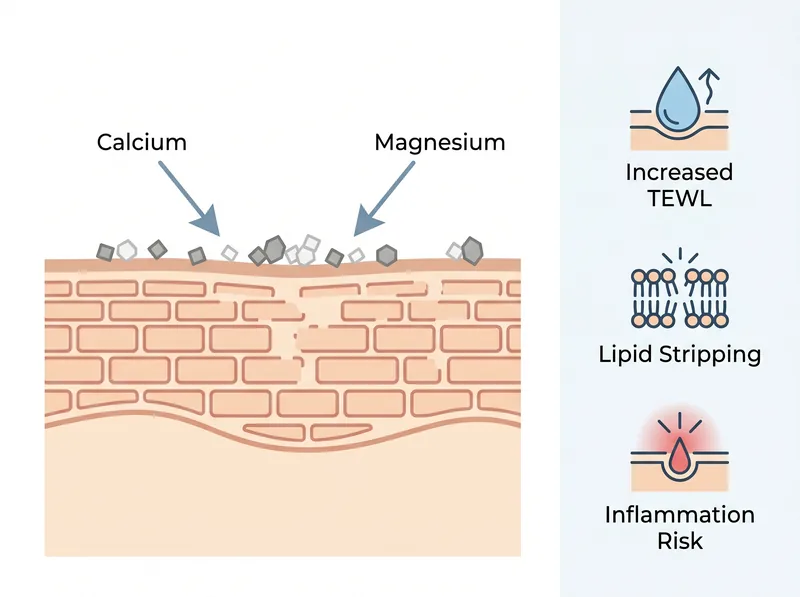 Hard water minerals compound the problem: they bind to an already-fragile barrier, stripping lipids and increasing trans-epidermal water loss.
Hard water minerals compound the problem: they bind to an already-fragile barrier, stripping lipids and increasing trans-epidermal water loss.
How Hard Water Turns Hormonal Skin Damage Into a Crisis
If you’re living in a hard water region, your skin is facing a double assault. The hormonal barrier collapse is bad enough. But hard water actively strips what’s left.
Hard water contains high concentrations of calcium and magnesium ions. When you wash your face, these minerals bind to the lipids in your already-compromised barrier. They form insoluble compounds, soap scum on your skin. This process, called chelation, pulls lipids away from the barrier structure. We’ve covered hard water’s effect on the skin barrier in detail before, but the impact is exponentially worse when your barrier is already hormonally weakened.
The minerals also deposit on the skin surface, creating a film that blocks moisture absorption and increases irritation. Your skin becomes reactive to products that never bothered you before. Redness, stinging, flaking, it’s not sensitivity, it’s barrier failure compounded by mineral buildup.
And because menopausal skin produces less sebum, you don’t have the natural oils to buffer the mineral assault. The barrier is exposed, fragile, and under constant attack every time you wash your face.
Why Standard Anti-Aging Advice Backfires on Menopausal Skin
Most anti-aging skincare is designed for skin that still has a functioning barrier. Retinoids, AHAs, vitamin C, these are powerful actives that work when your skin can tolerate them. But when your barrier is collapsing, they become irritants.
Retinol increases cell turnover and stimulates collagen production. Great in theory. But it also temporarily changes the barrier during the adjustment period. If your barrier is already compromised by estrogen loss, retinol can push it into full breakdown. The result: peeling, redness, and skin that looks worse, not better.
The same goes for exfoliating acids. AHAs and BHAs dissolve the bonds between dead skin cells, which is useful for congestion and texture. But they also strip lipids. On menopausal skin in a hard water climate, this is a disaster. You’re removing the only lipid protection you have left.
The skincare industry sells anti-aging as a singular goal. But for menopausal skin, barrier repair must come first. You can’t address collagen loss if your skin can’t hold water. You can’t tolerate actives if your barrier is in crisis. The hierarchy matters.
 A barrier-focused routine: gentle cleansing, lipid replenishment, and occlusive sealing to support compromised skin.
A barrier-focused routine: gentle cleansing, lipid replenishment, and occlusive sealing to support compromised skin.
What Actually Works: Barrier-First Skincare for Estrogen-Deficient Skin
The solution isn’t more expensive products. It’s a complete strategic shift toward barrier support. Your routine needs to do three things: cleanse without stripping, replenish the lipid structure, and seal moisture in.
Start with gentle cleansing. In hard water, this means using a chelating cleanser that binds to calcium and magnesium before they bind to your skin. A formula like Regrowth+ chelating shampoo works on the scalp, and the same chelation principle applies to facial cleansers, look for EDTA, citric acid, or gluconate-based formulas that prevent mineral deposition.
Next, rebuild the lipid barrier with targeted ingredients. You need ceramides (ideally a ceramide complex with types 1, 3, and 6), cholesterol, and fatty acids in the right ratio. Ceramides are the foundation of barrier repair, especially in dry climates where TEWL is already improved by low humidity.
Look for products that contain niacinamide (which stimulates ceramide production) and hyaluronic acid (which holds water in the dermis). But don’t rely on hyaluronic acid alone, it needs a sealed barrier to work. Without lipids, it just evaporates.
Finally, seal everything with an occlusive layer. This doesn’t mean heavy petroleum jelly (though that works). It means ingredients like squalane, shea butter, or dimethicone that create a protective film over the repaired barrier. At night, a thicker occlusive is essential. Your skin loses more water while you sleep, and menopausal skin can’t afford that loss.
The Role of Systemic Support: What You Can Control Beyond Topicals
Skincare can only do so much when the problem is hormonal. But there are systemic interventions that support skin structure from the inside.
Hormone replacement therapy (HRT) is the most direct intervention. Studies show that HRT can improve skin thickness, collagen content, and elasticity in postmenopausal women by restoring estrogen levels. But HRT isn’t right for everyone, and the decision requires consultation with a healthcare provider who understands your risk profile.
If HRT isn’t an option, phytoestrogens, plant compounds with weak estrogen-like activity, may offer modest benefits. Soy isoflavones, red clover, and flaxseed have been studied for skin effects. The evidence is mixed, but some women report improvements in skin hydration and elasticity. We’ve covered supplement strategies for Gulf conditions that include phytoestrogen sources.
Omega-3 fatty acids support the lipid barrier from within. Research on omega-3s shows they reduce inflammation and support cell membrane integrity. For menopausal skin, this translates to better barrier function and reduced sensitivity. Aim for 1-2 grams of combined EPA and DHA daily from fish oil or algae oil.
Hydration is critical, especially in extreme heat. Your water needs increase significantly in hot climates, and dehydration worsens TEWL. But drinking more water won’t fix a broken barrier, you need to seal the skin from the outside while hydrating from within.
When to Seek Professional Help: Red Flags That Need Medical Attention
Some skin changes during menopause are expected. But certain symptoms indicate a problem beyond normal hormonal shifts.
Persistent redness, burning, or stinging that doesn’t improve with barrier repair suggests rosacea or dermatitis, both of which become more common after menopause. These conditions require prescription treatment, topical metronidazole for rosacea, corticosteroids for dermatitis.
Sudden onset of severe dryness with scaling, especially on the lower legs, can indicate thyroid dysfunction. Hypothyroidism is common in perimenopausal women and causes profound skin dryness that doesn’t respond to moisturiser. A simple TSH blood test can rule this out.
New or changing moles, rough patches that don’t heal, or any persistent skin lesions warrant immediate dermatological evaluation. Skin cancer risk increases with age and cumulative sun exposure, and menopausal skin is more vulnerable.
If your skin barrier doesn’t improve after 6-8 weeks of consistent barrier-repair skincare, see a dermatologist. You may need prescription-strength ceramide formulations, or there may be an underlying condition, eczema, psoriasis, autoimmune disease, that’s being unmasked by hormonal changes.
Building a Realistic Routine for Menopausal Skin in Hard Water
Here’s what a functional routine looks like when you’re dealing with both hormonal barrier collapse and hard water damage.
Morning: Rinse with lukewarm water only, or use a chelating micellar water to remove overnight buildup without stripping. Apply a ceramide-rich serum to damp skin. Follow with a lightweight moisturiser containing niacinamide and hyaluronic acid. Finish with broad-spectrum SPF 50, mineral sunscreens (zinc oxide, titanium dioxide) are less irritating on compromised skin.
Evening: Cleanse with a gentle, chelating cream cleanser. If you’re using actives like retinol, apply them only 2-3 nights per week, and only after your barrier has stabilised. On non-active nights, layer a ceramide serum, a richer moisturiser, and an occlusive (squalane oil or a petrolatum-based balm) to seal everything in.
Weekly: Use a gentle enzyme mask (not a scrub) to remove dead skin buildup without mechanical abrasion. Avoid anything with high concentrations of acids until your barrier is fully repaired. If you’re in a very hard water area, consider installing a shower filter, it won’t remove all minerals, but it reduces chlorine and some calcium, which helps.
The goal isn’t perfection. It’s damage control. Your skin won’t look like it did at 35, and that’s not the point. The point is a barrier that functions, skin that doesn’t hurt, and a routine that works with your biology instead of fighting it.
References
- Skin ageing and menopause: implications for treatment - American Journal of Clinical Dermatology
- Epidermal lipid composition, barrier integrity, and eczematous inflammation are associated with skin microbiome configuration - Journal of Investigative Dermatology
- Hormone replacement therapy and skin aging: a systematic review - PubMed Central
- The role of ceramides in skin barrier function and the pathogenesis of atopic dermatitis - Journal of Clinical Medicine
- Menopause and the skin: old favorites and new innovations in cosmeceuticals for estrogen-deficient skin - Clinics in Dermatology