
Medically reviewed by Dr. Layla Hassan, Trichologist and Dermatology Consultant
If you’re over 40 and you’ve noticed that intimate skin feels different, drier, more reactive, or just not right anymore, you’re not imagining it. What’s happening isn’t about hygiene or what soap you’re using. It’s estrogen withdrawal, and it changes the entire structure of intimate tissue in ways most women aren’t warned about.
The tissue in the vulvar and vaginal area is estrogen-dependent. When estrogen declines during perimenopause and menopause, that tissue thins, loses elasticity, produces less natural moisture, and becomes more vulnerable to irritation and infection. The medical term is vulvovaginal atrophy, but that clinical label doesn’t capture how significant these changes can be to daily comfort, intimacy, and quality of life.
This isn’t a minor inconvenience. Research shows that up to 84% of postmenopausal women experience symptoms of vulvovaginal atrophy, yet fewer than 25% seek treatment. The gap between prevalence and treatment is massive, partly because women don’t know what’s normal, what’s fixable, and what their options are. Here’s what’s actually happening, what you can do about it, and what works.
What Estrogen Decline Does to Intimate Tissue
Estrogen isn’t just a reproductive hormone. It maintains the structure and function of mucous membranes throughout your body, including the vulva and vagina. When estrogen levels drop, the tissue changes in predictable, measurable ways.
The vaginal lining becomes thinner. What was once a thick, multi-layered epithelium becomes fragile and easily damaged. Blood flow to the area decreases, which reduces natural lubrication and slows tissue repair. Collagen and elastin production decline, so the tissue loses its stretch and resilience.
The pH of the vagina shifts from acidic (around 4.5) to more neutral (6.0 or higher). That pH change changes the balance of healthy bacteria, making you more susceptible to infections like bacterial vaginosis and urinary tract infections. The tissue also produces less glycogen, which feeds the protective lactobacilli that keep the vaginal environment stable.
All of this happens gradually. You might notice occasional dryness at first, then persistent discomfort, then pain during intercourse, then itching or burning that doesn’t go away. The progression can take years, but the underlying cause is the same: tissue that’s structurally different without estrogen support.
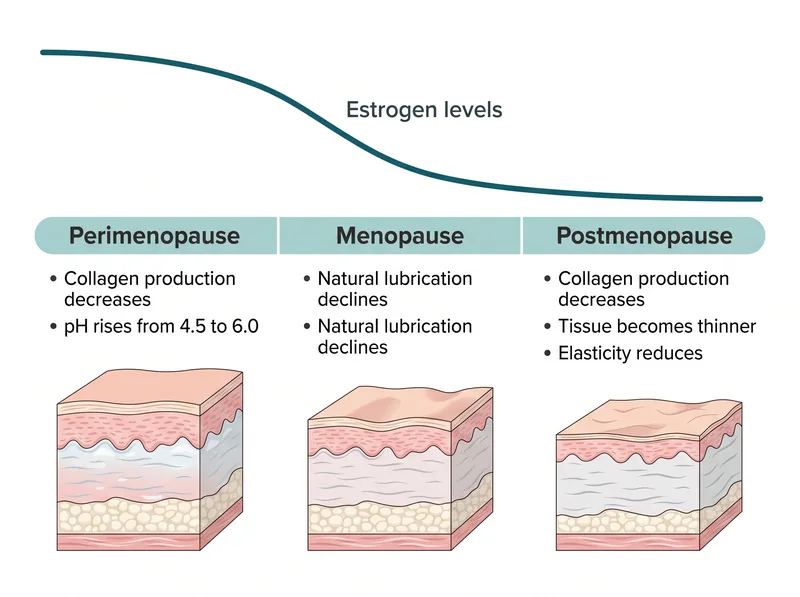 How declining estrogen affects intimate tissue structure and moisture levels across the menopause transition
How declining estrogen affects intimate tissue structure and moisture levels across the menopause transition
Symptoms That Signal Tissue Changes
Vaginal dryness is the most commonly reported symptom, but it’s not the only one. Many women describe a feeling of rawness or soreness even when they’re not doing anything. The vulvar skin can feel tight, thin, or papery. Some women notice a burning sensation when they urinate, or increased frequency and urgency.
Itching is common, and it’s often worse at night or after bathing. The skin can become so reactive that even water feels irritating. Some women develop recurrent infections (yeast, bacterial, or urinary) because the tissue’s protective barrier is compromised.
Pain during intercourse (dyspareunia) is another major symptom. The tissue doesn’t stretch the way it used to, and there’s not enough natural lubrication to reduce friction. For some women, this makes intimacy impossible without significant discomfort or even tearing.
These symptoms don’t improve on their own. Unlike hot flashes, which often resolve after menopause, vulvovaginal atrophy is progressive. Without intervention, the tissue continues to thin and become more fragile over time.
Medical Treatments That Actually Work
The most effective treatment for vulvovaginal atrophy is topical estrogen. This is not the same as systemic hormone replacement therapy. Topical estrogen (available as creams, tablets, or rings) delivers a very low dose of estrogen directly to the vaginal tissue, where it restores thickness, elasticity, and moisture without raising blood estrogen levels significantly.
Studies show that topical estrogen improves symptoms in 80-90% of women within a few weeks of starting treatment. It’s considered safe even for women who can’t take systemic HRT, including many breast cancer survivors, though you should always discuss your specific history with your doctor.
If estrogen isn’t an option, there are non-hormonal prescription treatments. Ospemifene (Osphena) is an oral medication that acts like estrogen on vaginal tissue without affecting breast or uterine tissue. Prasterone (Intrarosa) is a DHEA suppository that the body converts to estrogen locally in the vagina.
Over-the-counter vaginal moisturizers (like Replens or Hyalo Gyn) can provide temporary relief by adding moisture to the tissue, but they don’t reverse the structural changes. They’re useful for mild symptoms or as a supplement to other treatments, but they’re not a replacement for estrogen if you need it.
 Safe ingredient choices for intimate skincare, and what to avoid when tissue is more vulnerable
Safe ingredient choices for intimate skincare, and what to avoid when tissue is more vulnerable
What to Look for in Intimate Skincare Products
The vulvar skin is different from the skin on the rest of your body. It’s thinner, more permeable, and has a different pH. Products formulated for facial or body skin are often too harsh for this area, especially when tissue is already compromised by estrogen loss.
Look for products specifically labeled for intimate or vulvar use. These should be fragrance-free (both synthetic and natural fragrances can irritate), pH-balanced (around 4.5-5.5), and free of potential irritants like alcohol, glycolic acid, retinol, essential oils, and dyes.
Helpful ingredients include hyaluronic acid (which holds moisture in tissue), vitamin E (anti-inflammatory and healing), glycerin (a humectant that draws water into skin), squalane (a lightweight emollient), and colloidal oatmeal (soothing and barrier-repairing).
Avoid anything marketed as ‘tightening’, ‘brightening’, or ‘rejuvenating’ for intimate areas. These products often contain acids, retinoids, or other actives that can damage already vulnerable tissue. The goal is gentle support, not aggressive treatment.
Daily Care Practices That Help
How you wash matters more than what you wash with. Use lukewarm water only. You don’t need soap on the vulva; in fact, soap changes the natural pH and can worsen dryness. If you feel you must use a cleanser, choose one formulated for intimate use with a pH around 5.
Pat dry gently after washing. Don’t rub. If you’re very dry, you can apply a thin layer of a vulvar moisturizer while the skin is still slightly damp to lock in moisture. Products like Cetaphil or CeraVe (fragrance-free versions) can work, but dedicated vulvar moisturizers are often better tolerated.
Wear breathable cotton underwear and avoid tight clothing that traps heat and moisture. In hot climates like the Gulf, this is especially important. Synthetic fabrics and restrictive clothing can create an environment that promotes irritation and infection.
If you’re sexually active, use a lubricant every time. Even if you don’t feel dry, the tissue is more fragile than it used to be. Water-based or silicone-based lubricants work well; avoid anything with glycerin if you’re prone to yeast infections, and skip any lubricants with warming or cooling sensations, which are usually achieved with irritants like menthol.
When to See a Doctor
If you’re experiencing persistent dryness, pain, itching, or recurrent infections, see a healthcare provider. Many women wait years before seeking help, assuming these symptoms are just part of aging or that nothing can be done. That’s not true.
A gynecologist or menopause specialist can assess the tissue, rule out other conditions (like lichen sclerosus or lichen planus, which require different treatment), and prescribe appropriate therapy. Don’t accept ‘it’s just menopause’ as the end of the conversation if your symptoms are affecting your quality of life.
If you notice any unusual discharge, bleeding, sores, or lumps, get evaluated promptly. While most intimate skin changes in menopause are benign, it’s important to rule out conditions that need specific treatment.
You should also see a doctor if over-the-counter products aren’t helping after a few weeks, or if symptoms are getting worse despite your efforts. Vulvovaginal atrophy is progressive, and early intervention with prescription treatments can prevent more severe tissue changes down the line.
What Doesn’t Work (Despite the Marketing)
Vaginal steaming, jade eggs, and other wellness trends have no evidence supporting their use and can actually cause harm. Steaming can burn delicate tissue. Jade eggs can introduce bacteria and cause trauma.
Douching is never recommended. It changes the vaginal microbiome, raises pH, and increases infection risk. Your vagina is self-cleaning; you don’t need to rinse or flush it.
Oral collagen supplements are heavily marketed for vaginal health, but there’s no strong evidence they improve vaginal tissue specifically. Collagen is broken down in digestion; it doesn’t travel intact to rebuild vaginal collagen. Topical estrogen is far more effective.
Probiotics (oral or vaginal) may help maintain a healthy vaginal microbiome, but they don’t reverse tissue atrophy. They’re an adjunct, not a primary treatment. If your tissue is thinned and estrogen-depleted, probiotics alone won’t restore structure.
References
- Vaginal Atrophy (Atrophic Vaginitis): Symptoms, Causes, Treatment - Mayo Clinic
- Efficacy of Topical Estrogen Therapy in the Treatment of Vaginal Atrophy - PubMed Central
- Vaginal pH and Microbiota Changes During Menopause - PubMed Central
- Hyaluronic Acid in Dermatology and Tissue Repair - PubMed Central
- Genitourinary Syndrome of Menopause: Management Strategies - American College of Obstetricians and Gynecologists