
Your baby’s skin felt perfect at birth. Soft, smooth, resilient. Then you moved to the Gulf, or your baby was born here, and within weeks you noticed the changes. Dry patches on the cheeks. Rough texture on the arms. A persistent redness that your pediatrician can’t quite explain. You’ve switched lotions three times. You’re bathing less frequently. Nothing seems to help.
Here’s what most pediatricians in the region won’t tell you: the water itself might be the problem. This article contains affiliate links. See our affiliate disclosure for details.
The Gulf region has some of the hardest water in the world, with mineral concentrations that can exceed 400 parts per million. While adults struggle with this water quality, infant skin faces a unique vulnerability. Baby skin is 30% thinner than adult skin, with an underdeveloped barrier that allows minerals to penetrate more easily. What registers as mild dryness for you can manifest as eczema, irritation, or persistent inflammation for your baby.
This isn’t about being a better mother or finding the right product. It’s about understanding how environmental factors beyond your control affect your baby’s developing skin, and what you can actually do about it. Desalinated water, which supplies most Gulf households, strips away the natural minerals that normally buffer hardness, leaving behind a chemically aggressive solution that changes skin pH and moisture retention.
Why Infant Skin Reacts Differently to Hard Water
Infant skin isn’t just smaller adult skin. It’s structurally different in ways that make it more vulnerable to environmental stressors. The stratum corneum (the outermost protective layer) is significantly thinner in babies, and the lipid barrier that normally prevents water loss and blocks irritants is still developing during the first year of life.
When hard water contacts infant skin, several damaging processes occur simultaneously. Calcium and magnesium ions bind to the skin’s surface, forming insoluble deposits that physically change the lipid barrier. These mineral deposits create microscopic gaps in the skin’s protective layer, allowing water to evaporate more rapidly and irritants to penetrate more easily.
Research published in the Journal of Investigative Dermatology found that infants bathed in hard water (above 250 ppm) showed a 35% increase in transepidermal water loss compared to those bathed in soft water. This accelerated moisture loss triggers a cascade of inflammatory responses as the skin attempts to repair itself, often manifesting as the dry patches, redness, and rough texture you’re seeing.
The pH changeion is equally problematic. Infant skin naturally maintains a slightly acidic pH (around 5.5) that supports beneficial bacteria and discourages pathogens. Hard water, especially desalinated water common in Gulf households, typically has a pH between 7.5 and 8.5. Regular exposure to this alkaline water gradually shifts your baby’s skin pH, weakening its natural antimicrobial defenses and increasing susceptibility to bacterial and fungal infections.
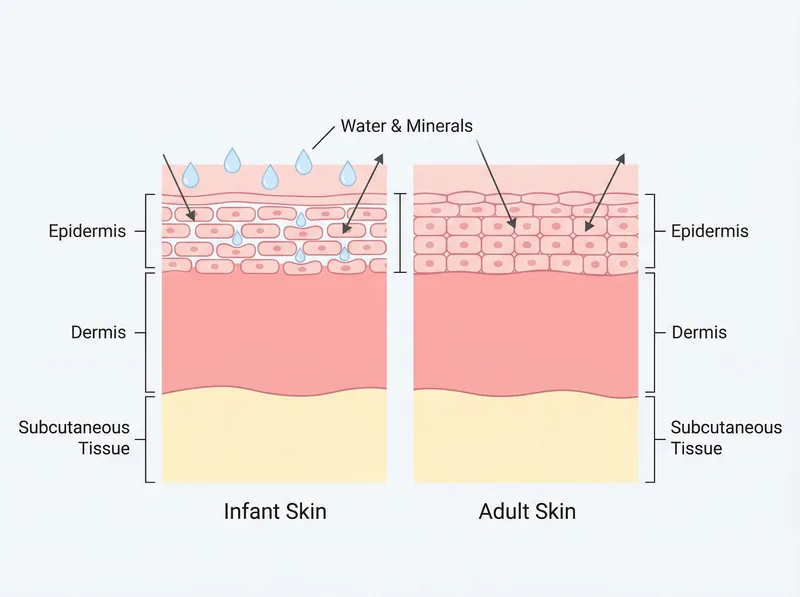 Infant skin is 30% thinner than adult skin, making it more vulnerable to environmental irritants like hard water minerals.
Infant skin is 30% thinner than adult skin, making it more vulnerable to environmental irritants like hard water minerals.
The Gulf Water Quality Factor
The water quality challenges in the Gulf region are uniquely severe. Most households receive desalinated seawater that’s been chemically treated to remove salt but retains high concentrations of calcium, magnesium, and sulfates. Unlike naturally soft water found in many other regions, this processed water lacks the trace minerals that normally help buffer its effects on skin.
A 2024 water quality study across Gulf municipalities found average hardness levels between 320-450 ppm (parts per million), with some areas exceeding 500 ppm. For context, water above 180 ppm is considered “very hard” by international standards. Your baby is being bathed in water that’s more than twice as harsh as what’s considered problematic in most developed countries.
The chlorination levels compound the issue. Gulf water typically contains 0.5-1.0 mg/L of residual chlorine to prevent bacterial growth in the distribution system. While this keeps water safe to drink, it adds another layer of chemical stress to infant skin. Chlorine strips natural oils, oxidizes lipids in the skin barrier, and can trigger allergic reactions in sensitive babies.
Temperature extremes matter too. During Gulf summers, water sitting in building tanks and pipes can reach 40-45°C before it even reaches your tap. This heat accelerates mineral precipitation, meaning the water that touches your baby’s skin carries even higher concentrations of dissolved solids than the municipal supply. The extreme heat also means babies lose more moisture through perspiration, making the barrier-changeing effects of hard water even more damaging.
Recognizing Hard Water Damage on Infant Skin
The symptoms of hard water exposure in babies often get misdiagnosed as eczema, allergies, or “sensitive skin.” Learning to recognize the specific patterns helps you address the root cause rather than just treating symptoms.
The first sign is usually persistent dryness that doesn’t respond to moisturizing. You apply lotion after every bath, maybe even between baths, but your baby’s skin feels rough and looks dull within hours. This happens because the mineral film on the skin prevents moisturizers from penetrating properly. You’re essentially trying to hydrate through a mineral barrier.
Red, irritated patches typically appear in areas where water pools during bathing: the creases of the neck, behind the ears, in the elbow and knee folds. These areas stay damp longer, giving minerals more time to deposit and change the barrier. The irritation often worsens after bath time rather than improving, which is the opposite of what should happen with proper bathing.
Rough, sandpaper-like texture on the arms, legs, or cheeks indicates keratosis pilaris, a condition where dead skin cells and minerals clog hair follicles. While KP has genetic components, hard water dramatically worsens it by preventing normal skin cell turnover. The condition is significantly more common in Gulf-based infants than in babies living in soft water regions.
Persistent cradle cap that doesn’t respond to typical treatments may also be hard-water related. The mineral deposits on the scalp create an environment where yeast (Malassezia) thrives, leading to the thick, yellowish scales characteristic of seborrheic dermatitis. Standard treatments fail because they don’t address the underlying mineral buildup.
 Testing water temperature and quality before bathing helps protect your baby’s sensitive skin from both heat and mineral exposure.
Testing water temperature and quality before bathing helps protect your baby’s sensitive skin from both heat and mineral exposure.
Protective Bathing Strategies for Babies
The conventional advice to “bathe your baby daily” needs modification in hard water environments. Frequent bathing in mineral-heavy water does more harm than good, repeatedly stripping the skin barrier before it can recover.
Reduce bathing frequency to 2-3 times per week for infants under six months, focusing on spot-cleaning with a soft, damp cloth between full baths. Babies don’t get dirty the way older children do. They need cleansing around the diaper area and any milk or food residue, but full-body immersion in hard water isn’t necessary daily.
When you do bathe, keep it brief. Five minutes maximum. The longer your baby’s skin is exposed to hard water, the more minerals deposit and the more natural oils get stripped. Fill the tub with just enough water to keep your baby warm and supported, not deep enough for prolonged soaking.
Water temperature matters more than you might think. Keep bath water lukewarm (32-35°C), tested with your elbow or a thermometer. Hot water opens pores and softens the skin barrier, allowing minerals to penetrate more easily. It also accelerates moisture loss. What feels soothingly warm to you is often too hot for your baby’s thinner, more permeable skin.
Consider using filtered or bottled water for the final rinse, especially if your baby has active eczema or severe dryness. After washing with regular tap water, pour 1-2 liters of filtered water over your baby’s body to rinse away mineral residue before patting dry. This single step can dramatically reduce mineral deposits without requiring a whole-house filtration system.
Choosing the Right Cleansing Products
Not all baby washes are created equal, and what works in soft water regions often fails in hard water environments. The key is understanding how different formulations interact with mineral-heavy water.
Avoid traditional soaps entirely. True soap (sodium or potassium salts of fatty acids) reacts with calcium and magnesium to form insoluble deposits called soap scum. This scum doesn’t just stick to your bathtub; it coats your baby’s skin, clogging pores and preventing moisture absorption. Even “gentle” baby soaps cause this reaction in hard water.
Look for synthetic detergent-based (syndet) cleansers specifically formulated for hard water. These products use surfactants that don’t react with minerals, so they rinse clean without leaving residue. The ingredient list should include terms like sodium cocoyl isethionate, sodium lauroyl sarcosinate, or disodium laureth sulfosuccinate rather than saponified oils.
Chelating ingredients help too. Products containing EDTA (ethylenediaminetetraacetic acid), citric acid, or gluconates actively bind to calcium and magnesium ions, preventing them from depositing on skin. A chelating baby wash like Regrowth+ (originally formulated for hard water hair care but gentle enough for sensitive baby skin when diluted) can remove existing mineral buildup while preventing new deposits.
Fragrance-free is non-negotiable. Fragrances are among the most common allergens in baby products, and babies already dealing with barrier damage from hard water are more susceptible to sensitization. The “baby powder” or “lavender” scent isn’t worth the increased risk of allergic reactions.
Post-Bath Barrier Repair
What you do in the three minutes after bathing matters as much as the bath itself. This is your window to lock in moisture and repair the barrier damage caused by hard water exposure.
Pat dry, never rub. Use a soft cotton towel to gently press water from your baby’s skin, leaving it slightly damp. Rubbing creates friction that further damages the already-compromised barrier and can spread minerals across the skin surface.
Apply moisturizer within three minutes of bathing, while skin is still damp. This timing is critical. The stratum corneum is most permeable immediately after water exposure, allowing moisturizing ingredients to penetrate deeply. Wait longer, and you’ve missed the optimal window for barrier repair.
Choose occlusive moisturizers that create a physical barrier against moisture loss. Look for products containing petrolatum, dimethicone, or ceramides as primary ingredients. These occlusives sit on top of the skin, preventing the accelerated water loss that hard water triggers. Lighter lotions with humectants (like glycerin or hyaluronic acid) aren’t enough on their own; they draw moisture from the environment, but in dry Gulf climates with damaged barriers, there’s no moisture to draw.
Layer strategically in problem areas. For babies with eczema or severe dryness, apply a thin layer of barrier repair cream (containing ceramides or colloidal oatmeal) first, then seal it with a thicker occlusive like petroleum jelly. This two-step approach addresses both the barrier damage and the moisture loss.
When to Seek Professional Help
Most hard water-related skin issues in babies resolve with environmental modifications and proper skincare. But some situations require medical evaluation, and knowing the difference prevents complications.
Seek immediate medical attention if you notice signs of infection: oozing, crusting, or honey-colored discharge from irritated areas; fever accompanying skin symptoms; or red streaks extending from a rash. These indicate bacterial infection, which babies with compromised skin barriers are more susceptible to developing.
Persistent eczema that doesn’t improve after four weeks of consistent barrier protection and moisturizing needs professional assessment. Your pediatrician or a pediatric dermatologist can prescribe topical medications that reduce inflammation while you address the environmental triggers. Chronic inflammation can lead to skin thickening and permanent changes if left untreated.
Severe reactions to bathing (immediate redness, hives, or respiratory symptoms) suggest an allergy rather than simple hard water irritation. This requires allergy testing to identify specific triggers, whether in the water treatment chemicals or the products you’re using.
Don’t hesitate to advocate for your baby with healthcare providers who may not be familiar with hard water’s effects. Many pediatricians, especially those trained in soft-water regions, don’t recognize mineral exposure as a primary cause of infant skin problems. Bring documentation of your water hardness (available from your municipality or through home testing kits) to help them understand the environmental context.
References
- Hard Water Exposure and Eczema Development in Infants: A Population-Based Study - Journal of Investigative Dermatology
- Infant Skin Care and Development - American Academy of Dermatology
- Guidelines for Drinking-Water Quality: Fourth Edition - World Health Organization
- Atopic Dermatitis (Eczema) in Infants - Mayo Clinic
- Effects of Desalinated Water on Skin Barrier Function - PubMed Central