
If you’ve been told your hair loss is thyroid-related, you’ve probably noticed something confusing: the advice you’re reading online doesn’t match what you’re seeing in the mirror. That’s because hypothyroid hair loss and hyperthyroid hair loss look completely different. They shed differently, they feel different, and they respond to treatment differently.
This article contains affiliate links. See our affiliate disclosure for details.
The confusion isn’t your fault. Most articles lump all thyroid hair loss into one category, as if an underactive thyroid and an overactive thyroid cause the same problem. They don’t. One causes slow, coarse, brittle thinning. The other causes rapid, fine, diffuse shedding. And if you’re treating the wrong pattern, you’re wasting time on solutions that won’t work.
Here’s what makes this particularly relevant if you’re living in a hard water climate: once your thyroid is treated and your levels are stable, environmental factors like hard water mineral buildup become the fixable variable that’s still sabotaging your regrowth. Many women get their TSH into range, expect their hair to recover, and then can’t understand why it’s still struggling. The answer is often sitting in their shower water.
Key Takeaways
• Hypothyroid hair loss is slow, coarse, and brittle with characteristic outer eyebrow thinning, while hyperthyroid hair loss is rapid, fine, and diffuse across the entire scalp.
• TSH levels below 0.5 mIU/L or above 4.5 mIU/L both correlate with increased shedding, but the texture and pattern differ significantly between the two conditions.
• Thyroid hair loss is reversible with proper treatment, but recovery can take 6-12 months as the hair growth cycle resets.
• Environmental factors like hard water mineral buildup can prevent regrowth even after thyroid levels normalize, requiring targeted scalp preparation.
• Always work with an endocrinologist for thyroid management; hair loss is a symptom, not the primary concern, and self-treatment is dangerous.
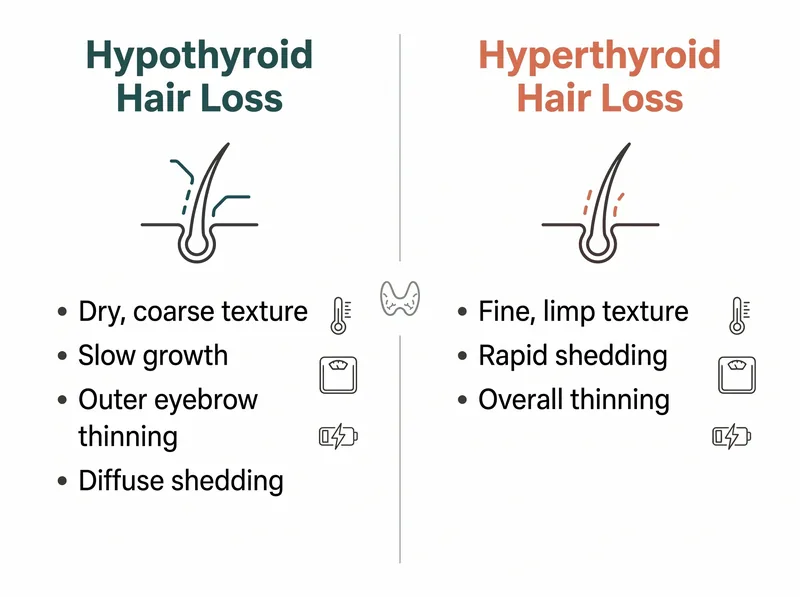 Hypothyroid and hyperthyroid hair loss present with distinctly different patterns and accompanying symptoms.
Hypothyroid and hyperthyroid hair loss present with distinctly different patterns and accompanying symptoms.
How Hypothyroid Hair Loss Actually Looks
Hypothyroid hair loss is characterised by slow, progressive thinning that feels dry and coarse to the touch. The hair doesn’t shed in dramatic clumps. Instead, it grows more slowly, breaks more easily, and gradually becomes sparse over months or years. The texture changes first. Your hair feels rough, straw-like, resistant to styling.
The telltale sign is outer eyebrow thinning. If the outer third of your eyebrows has disappeared while the inner portion remains intact, that’s a classic hypothyroid pattern. It’s not universal, but it’s common enough that dermatologists look for it during thyroid-related hair loss assessments.
Shedding is diffuse but not alarming. You won’t see handfuls in the shower. You’ll notice your ponytail is thinner, your part is wider, your scalp is more visible. The hair that does grow tends to be fine and fragile, breaking at the mid-shaft rather than shedding from the root. This is because low thyroid hormone levels change the anagen (growth) phase, shortening the time your hair spends actively growing.
Women with Hashimoto’s thyroiditis often experience this pattern, sometimes for years before diagnosis. The hair loss is gradual enough that you might attribute it to aging, stress, or postpartum recovery, especially if you’re not experiencing the more obvious hypothyroid symptoms like weight gain or fatigue.
How Hyperthyroid Hair Loss Actually Looks
Hyperthyroid hair loss is fast, alarming, and impossible to ignore. The shedding is dramatic. You’ll see it in the shower drain, on your pillow, all over your clothes. This isn’t the gradual thinning of hypothyroidism. This is acute telogen effluvium triggered by metabolic overdrive.
The hair itself feels fine and limp, not coarse. It lacks body, won’t hold a style, and seems to slide out of hair ties. The texture is soft but weak, breaking easily under minimal tension. Unlike hypothyroid hair, which breaks at the mid-shaft, hyperthyroid hair sheds from the root, coming out in complete strands with the white bulb still attached.
The pattern is diffuse across the entire scalp. There’s no characteristic eyebrow loss, no specific thinning zone. Everything sheds at once. The scalp may feel tender or sensitive, and some women report a burning or tingling sensation, though this isn’t universal. The shedding often begins 2-3 months after thyroid hormone levels spike, following the natural telogen effluvium timeline.
If you have Graves’ disease or are taking too much thyroid replacement medication, this is the pattern you’ll see. The good news is that it’s highly responsive to treatment. Once thyroid levels normalise, the shedding stops relatively quickly, though regrowth takes the usual 6-12 months.
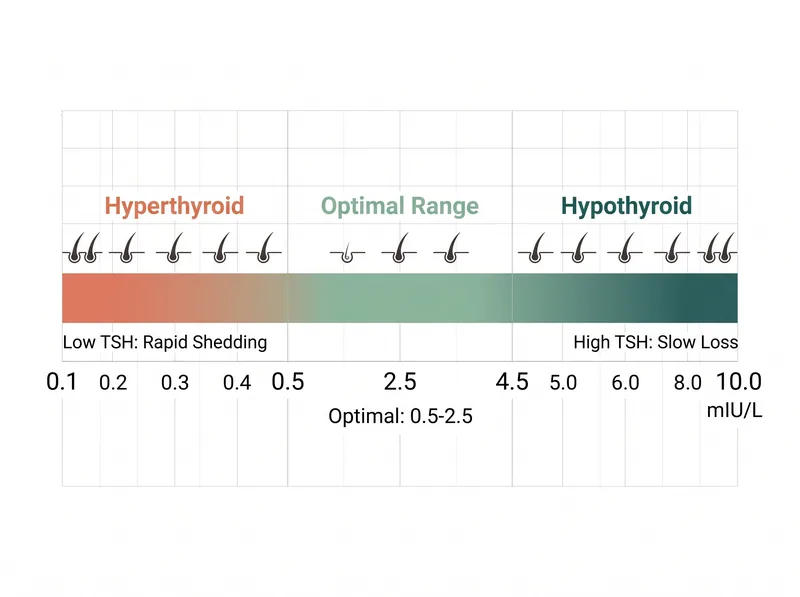 TSH levels outside the optimal range correlate with increased hair shedding, but the pattern differs between hypothyroid and hyperthyroid states.
TSH levels outside the optimal range correlate with increased hair shedding, but the pattern differs between hypothyroid and hyperthyroid states.
Why TSH Levels Matter More Than You Think
TSH (thyroid-stimulating hormone) is the blood marker most doctors use to assess thyroid function, and it’s the single most important number for understanding your hair loss pattern. Normal TSH ranges from about 0.4 to 4.5 mIU/L, but optimal for hair health appears to be between 0.5 and 2.5 mIU/L. Outside that range, hair suffers.
When TSH is high (above 4.5), it signals hypothyroidism. Your thyroid isn’t producing enough hormone, so your pituitary gland pumps out more TSH trying to stimulate it. Hair growth slows, texture coarsens, and shedding becomes chronic but gradual. When TSH is low (below 0.5), it signals hyperthyroidism. Your thyroid is overproducing, so your pituitary stops sending TSH signals. Hair sheds rapidly in response to the metabolic chaos.
Here’s what frustrates women: you can have a TSH within the normal lab range and still experience hair loss. A TSH of 3.8 is technically normal, but it’s high enough to cause symptoms in many women. Similarly, a TSH of 0.6 is normal, but some women shed heavily at that level. This is why endocrinologists often adjust medication based on symptoms, not just lab values.
If your hair loss started after beginning thyroid medication, your dose may be too high, pushing you into subclinical hyperthyroidism. If it started despite being on medication, your dose may be too low, leaving you subclinically hypothyroid. Both scenarios cause shedding, but the patterns differ. This is why regular monitoring and dose adjustment are critical.
Other Thyroid Symptoms That Accompany Hair Loss
Hair loss rarely appears in isolation. If it’s truly thyroid-related, you’ll have other symptoms, and recognising the cluster helps differentiate hypothyroid from hyperthyroid patterns. Hypothyroid symptoms include unexplained weight gain despite normal eating, persistent fatigue that doesn’t improve with sleep, cold intolerance (you’re freezing when everyone else is comfortable), constipation, dry skin, and brain fog. Your periods may become heavier or irregular.
Hyperthyroid symptoms are the opposite: unintentional weight loss despite eating normally, anxiety or irritability, heat intolerance, rapid heartbeat or palpitations, trembling hands, increased sweating, and diarrhoea. Your periods may become lighter or stop entirely. Some women develop a visible goiter (swelling at the base of the neck) or eye changes if Graves’ disease is the cause.
If you’re experiencing hair loss without any of these accompanying symptoms, thyroid dysfunction is less likely to be the primary cause. You may be dealing with iron deficiency, chronic stress, or environmental factors instead. Blood work is the only way to know for certain, which is why self-diagnosis based on hair loss alone is unreliable.
It’s also worth noting that thyroid dysfunction can coexist with other conditions. Women with PCOS, autoimmune conditions, or perimenopause often have thyroid issues as well, making the diagnostic picture more complex. This is why a full hormone panel, not just TSH, is essential for accurate assessment.
How Long Recovery Takes After Treatment Starts
Once your thyroid levels are corrected, hair loss doesn’t stop immediately. The hair growth cycle has its own timeline, and it doesn’t speed up just because your TSH is now optimal. You’re looking at 6-12 months before you see meaningful regrowth, and that assumes your thyroid stays stable during that period.
Here’s why: hair grows in cycles. The anagen (growth) phase lasts 2-7 years, the catagen (transition) phase lasts 2-3 weeks, and the telogen (resting) phase lasts 2-4 months. When thyroid dysfunction triggers shedding, it pushes a large percentage of follicles into telogen simultaneously. Even after treatment begins, those hairs will still shed on schedule. New growth only becomes visible after the follicles reset and re-enter anagen.
For hypothyroid hair loss, improvement is gradual. The texture normalises first. Your hair stops feeling so dry and brittle. Then growth speed picks up. Finally, density improves as new hairs fill in the thinned areas. For hyperthyroid hair loss, the shedding stops more abruptly once levels stabilise, but regrowth follows the same slow timeline. You’ll notice less hair in the drain before you notice more hair on your head.
This is where environmental factors become critical. If you’re living in a hard water area, mineral buildup on the scalp can physically block follicles and prevent new growth from emerging, even though your thyroid is now fine. Using a chelating shampoo like Regrowth+ to remove calcium and magnesium deposits gives your recovering follicles the best chance to function normally. Many women find that addressing the water quality issue is what finally allows their hair to recover after thyroid treatment.
When to Suspect Your Thyroid Despite Normal Labs
Standard thyroid panels often miss subclinical dysfunction, particularly in women whose symptoms don’t align with their TSH levels. If your TSH is normal but you’re experiencing classic thyroid hair loss patterns plus other symptoms, request a full thyroid panel: TSH, Free T3, Free T4, and thyroid antibodies (TPO and TgAb). Many women with Hashimoto’s have normal TSH but improved antibodies, indicating autoimmune attack even before thyroid function declines measurably.
Reverse T3 is another marker worth checking if standard labs are inconclusive. High reverse T3 can block thyroid hormone from working properly at the cellular level, causing hypothyroid symptoms despite normal TSH and Free T4. This is particularly common in women under chronic stress or dealing with improved cortisol levels.
Timing matters too. Thyroid function can fluctuate, especially in the early stages of autoimmune thyroid disease. A normal result today doesn’t mean your levels were normal three months ago when the hair loss started. If symptoms persist, retest every 6-8 weeks until you have a clear pattern. Some endocrinologists recommend testing first thing in the morning, as TSH levels vary throughout the day.
If you’ve recently moved to a new climate or are experiencing significant life stress, your thyroid may be struggling even if it was previously stable. The combination of environmental stressors and hormonal shifts can tip a borderline thyroid into dysfunction, triggering the hair loss that brought you here in the first place.
Why Hard Water Complicates Thyroid Hair Recovery
Even with perfect thyroid management, hair recovery can stall if you’re washing in hard water. Calcium and magnesium minerals bind to the hair shaft and scalp, creating a coating that prevents moisture absorption and blocks follicle openings. For women recovering from thyroid-related hair loss, this is particularly problematic because the new growth is already fragile and vulnerable.
Hypothyroid hair, which is already dry and brittle, becomes even more damaged when coated with mineral deposits. The hair can’t absorb conditioning treatments, so it remains rough and prone to breakage. Hyperthyroid hair, which is fine and weak, becomes weighed down and limp under mineral buildup, making the thinning look worse than it actually is. In both cases, the scalp environment becomes hostile to new growth.
This is especially relevant if you’re living in the Gulf region, parts of Australia, or the southwestern United States, where water hardness levels often exceed 300 ppm. The combination of thyroid-related hair fragility and aggressive mineral buildup creates a compounding problem that topical treatments alone can’t fix. You need to address the water chemistry directly.
Regular use of a chelating shampoo removes the mineral coating, allowing your scalp to function normally and your hair to absorb the treatments you’re using. For women whose thyroid levels are now stable but whose hair still isn’t recovering, this is often the missing piece. The mineral buildup was masking the improvement that should have been happening.
References
- Thyroid Hormones and Hair Follicle Biology - PubMed - Journal of Clinical Endocrinology & Metabolism
- Thyroid Dysfunction and Hair Disorders: A Narrative Review - PubMed Central
- TSH Test: Normal Ranges and Clinical Interpretation - Mayo Clinic
- Hair Loss and Thyroid Disease - American Academy of Dermatology
- Subclinical Thyroid Dysfunction and Hair Loss in Women - PubMed - Endocrine Practice