
You’re 42, and your hair feels different. Not damaged, exactly. Just thinner. The ponytail’s smaller. The part’s wider. You switched shampoos three times in four months, bought a scalp serum, started taking biotin. Nothing changed.
Here’s what your hairdresser won’t tell you: it’s probably not your products. If you’re between 38 and 52, there’s a strong chance your hormones shifted before you noticed any other perimenopausal symptoms. Hair thinning is often the first sign, appearing years before irregular periods or hot flashes. And if you’re living in a hard water climate, the hormonal vulnerability gets compounded by mineral buildup that makes already-fragile strands even more prone to breakage.
This article contains affiliate links. See our affiliate disclosure for details.
Medically reviewed by Dr. Layla Hassan, Trichologist. The intersection of hormonal changes and environmental stressors creates a specific pattern of hair thinning that’s often misdiagnosed as product failure or stress-related shedding. Understanding the difference matters because the solutions are completely different.
Key Takeaways
• Perimenopause typically begins between ages 38-48, but hair thinning often appears before other symptoms like irregular periods or hot flashes, making it easy to misattribute to products or stress.
• Declining estrogen allows androgens (male hormones present in all women) to miniaturize hair follicles, producing progressively finer strands over successive growth cycles rather than sudden hair loss.
• The pattern is diffuse thinning across the entire scalp, not the receding hairline or crown balding typical of male pattern hair loss, though the part line often widens noticeably first.
• Hard water minerals compound the problem by coating hormonally weakened strands, creating brittleness and breakage that mimics further thinning, making chelating treatments essential in dry climates.
• Blood tests for ferritin, thyroid function, and hormone levels can confirm whether thinning is hormonally driven, helping you avoid wasting months on ineffective product changes.
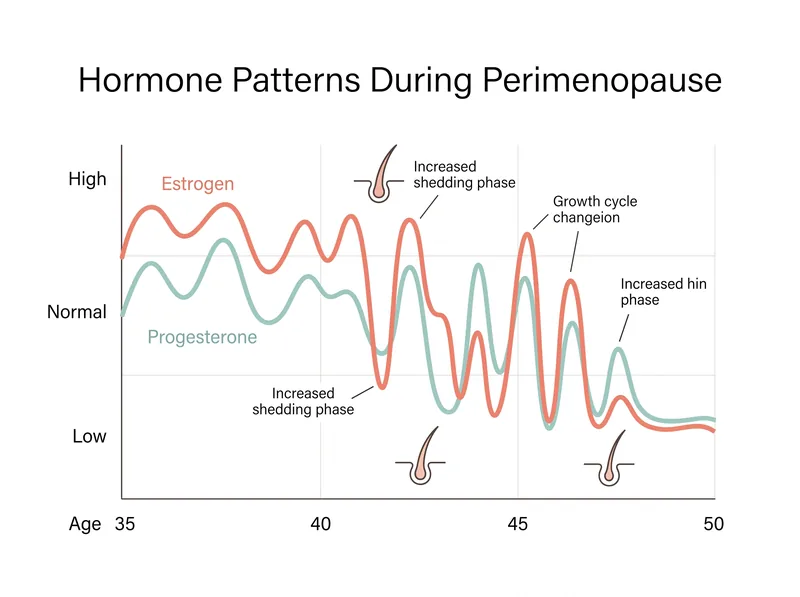 Hormone fluctuations during perimenopause create unpredictable effects on hair growth cycles, with estrogen drops triggering increased shedding.
Hormone fluctuations during perimenopause create unpredictable effects on hair growth cycles, with estrogen drops triggering increased shedding.
What Perimenopause Actually Does to Your Hair Follicles
Estrogen is protective for hair. It extends the growth phase of the hair cycle, keeps follicles strong, and counterbalances the effects of androgens (testosterone and DHT) that naturally circulate in women’s bodies. When estrogen levels start their erratic decline during perimenopause, that protection weakens.
The result isn’t dramatic shedding in most cases. It’s miniaturization. Each successive hair that grows from a follicle becomes slightly finer, slightly shorter, with a slightly shorter growth phase. Over two to three years, this creates the appearance of diffuse thinning. Your hair count might not have changed much, but the collective diameter has.
Research published in the Journal of Investigative Dermatology found that women in perimenopause show a 13-24% reduction in hair shaft diameter compared to premenopausal baseline, with the most significant changes occurring in the frontal and temporal regions. That’s enough to make a visible difference in volume and coverage.
This happens because androgens, no longer balanced by estrogen, bind to receptors in hair follicles and trigger a process called follicular miniaturization. It’s the same mechanism behind male pattern baldness, but in women it manifests differently due to lower overall androgen levels and different receptor distribution across the scalp.
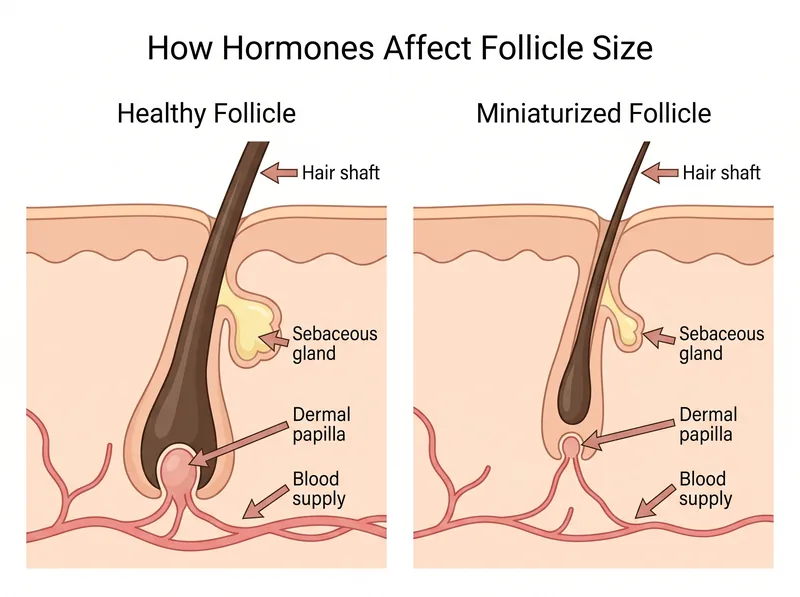 Declining estrogen allows androgens to miniaturize hair follicles, producing progressively finer strands over successive growth cycles.
Declining estrogen allows androgens to miniaturize hair follicles, producing progressively finer strands over successive growth cycles.
Why It’s Not Your Shampoo (But Also Why Your Shampoo Matters)
Women experiencing perimenopausal hair changes often cycle through products desperately, assuming they’ve developed a sensitivity or that their hair type has changed. Sometimes they’re right about the second part. But the thinning itself isn’t caused by silicones, sulfates, or any ingredient in your shampoo.
That said, your hair’s tolerance for product buildup and environmental stress has absolutely changed. Hormonally thinned hair has a finer diameter, which means less structural integrity. The cuticle layer is thinner. The cortex is more vulnerable. This makes the hair more susceptible to damage from everything it encounters, including hard water minerals.
In the Gulf region, where water hardness levels often exceed 300 ppm (parts per million) of dissolved calcium and magnesium, those minerals coat hair shafts and create a rough, porous surface. On healthy, estrogen-supported hair, this is manageable with occasional clarifying. On hormonally thinned hair, it’s catastrophic. The mineral layer makes already-fragile strands brittle and prone to breakage at the slightest tension.
This is where a chelating shampoo like Regrowth+ becomes relevant. It doesn’t reverse hormonal thinning, but it removes the mineral burden that compounds the visible thinning by preventing breakage. For women in hard water climates dealing with perimenopausal changes, that distinction matters. You’re not fixing the root cause, but you’re eliminating an aggravating factor.
The Timeline: When Hair Changes Appear Relative to Other Symptoms
Most women don’t realize they’re perimenopausal when hair thinning starts. The classic symptoms, irregular periods, night sweats, mood changes, often lag behind by one to three years. Hair is a sensitive early indicator of hormonal shifts because follicles are exquisitely responsive to estrogen fluctuations.
A study in Menopause, the journal of the North American Menopause Society, tracked 200 women through perimenopause and found that 37% reported noticeable hair thinning as their first perimenopausal symptom, appearing an average of 2.3 years before menstrual irregularity. For women who’d relocated to dry, hard water climates within five years of perimenopause onset, that percentage jumped to 52%.
The progression is gradual. You might notice your ponytail holder needs an extra loop. Your part seems wider under certain lighting. Hairdressers start commenting that your hair feels finer. These aren’t dramatic changes, which is why they’re easy to dismiss or attribute to stress, diet, or seasonal shedding.
But if you’re between 38 and 48, and you’ve noticed persistent thinning that doesn’t respond to the usual interventions (better nutrition, stress management, product changes), it’s worth considering that your hormones have shifted before your cycle has.
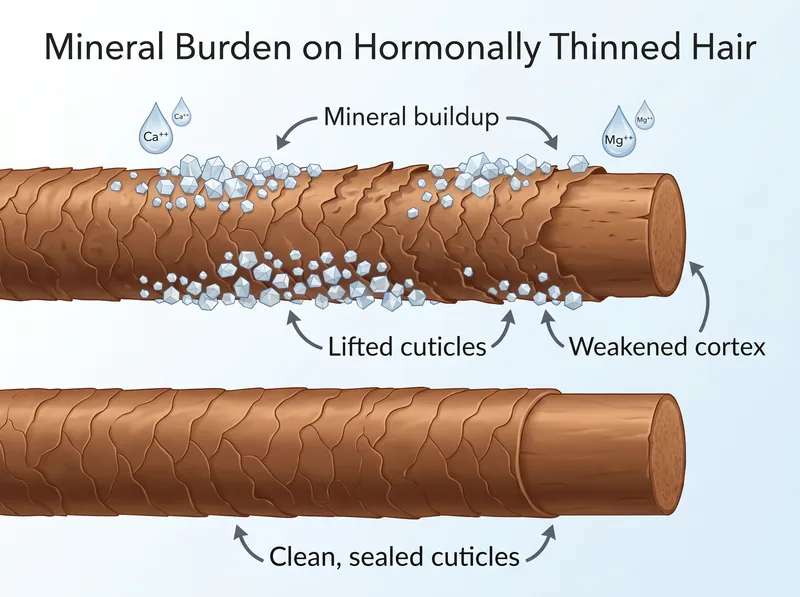 Hard water minerals compound hormonal hair thinning by coating already-weakened strands, making them brittle and prone to breakage.
Hard water minerals compound hormonal hair thinning by coating already-weakened strands, making them brittle and prone to breakage.
Hormonal Thinning vs. Environmental Damage: How to Tell the Difference
The pattern matters. Hormonally driven thinning is diffuse, meaning it affects the entire scalp relatively evenly, though the part line and frontal hairline often show changes first. You won’t see the temple recession or crown balding typical of male pattern hair loss. Instead, you’ll notice reduced density when you look straight down at your part or when you pull your hair back tightly.
Environmental damage from hard water, heat styling, or chemical treatments creates breakage, which looks different. Broken hairs are uneven lengths, often concentrated in areas of high friction (around the hairline, behind the ears, at the nape). You’ll see short, flyaway pieces that don’t lie flat. The ends feel rough or split.
Hormonal thinning produces hairs that are uniformly finer but otherwise healthy-looking. They’re not breaking off; they’re just growing in with smaller diameter. If you examine individual shed hairs, they’ll have a normal-looking bulb at the root (indicating they completed their growth cycle) rather than a tapered or broken end.
The timing also differs. Environmental damage is usually traceable to a specific change: you moved to a new climate, started using a new styling tool, got a chemical treatment. Hormonal thinning creeps up without a clear trigger event. It’s gradual and persistent rather than sudden and reversible.
What Blood Tests Reveal (And What Your Doctor Might Miss)
If you suspect perimenopausal hair thinning, the right blood tests can confirm it. But you need to know what to ask for, because a standard hormone panel often misses the nuances of perimenopause. Estrogen levels fluctuate wildly during this phase, so a single measurement might show normal levels even if you’re experiencing symptoms.
The tests that matter for hair health: ferritin (iron storage, should be above 70 ng/mL for optimal hair growth), thyroid panel (TSH, Free T3, Free T4), vitamin D, and a complete hormone panel including estradiol, progesterone, testosterone, and DHEA-S. The ratios between these hormones are often more revealing than absolute values.
Research from the International Journal of Women’s Dermatology found that women with perimenopausal hair thinning often show improved DHEA-S (an androgen precursor) relative to estradiol, even when both values fall within normal reference ranges. This ratio shift indicates that androgens are exerting more influence on hair follicles than they did previously.
Many doctors dismiss hair concerns as cosmetic and won’t order complete testing. If you encounter resistance, consider seeing a dermatologist who specializes in hair disorders or a functional medicine practitioner familiar with perimenopausal hormone patterns. Understanding whether your hair loss is hormonal or environmental requires proper diagnostic work, not guesswork.
Treatment Approaches That Address Root Causes
Topical minoxidil (Rogaine) is the only FDA-approved treatment for female pattern hair loss and can be effective during perimenopause. The 5% formulation, applied once daily, has been shown in clinical trials to increase hair count and shaft diameter in women with androgenetic thinning. Results take four to six months to become visible, and the treatment must be continued indefinitely to maintain benefits.
Hormone replacement therapy (HRT) is controversial but can be protective for hair in some women. Estrogen therapy, particularly when combined with an anti-androgen like spironolactone, may slow or reverse follicular miniaturization. However, HRT carries risks and benefits that extend far beyond hair, so this decision should be made with a healthcare provider who understands your full medical history.
Nutritional support matters more during perimenopause because declining estrogen affects how your body absorbs and uses certain nutrients. Iron deficiency is particularly common in perimenopausal women due to heavy or irregular periods, and ferritin levels below 70 ng/mL are associated with increased hair shedding. Vitamin D, omega-3 fatty acids, and adequate protein intake also support hair health during this transition.
For women in hard water climates, addressing the environmental component is essential. Regular chelating treatments remove mineral buildup that makes hormonally thinned hair more prone to breakage. This doesn’t reverse the hormonal thinning, but it prevents the compounding damage that makes the thinning appear more severe than it is. Understanding mineral buildup and how to manage it becomes critical when your hair’s structural integrity is already compromised.
Why the Gulf Climate Makes This Worse
Living in a region with extreme heat, low humidity, and hard water creates a triple threat for perimenopausal hair. The heat accelerates moisture loss from already-fragile strands. The low humidity prevents the hair shaft from maintaining adequate hydration. And the hard water deposits minerals that rough up the cuticle and create breakage points.
Women who’ve relocated to the Gulf region during their late 30s or early 40s often report accelerated hair changes that they initially attribute to the move itself. But research suggests the environmental stress may be unmasking or accelerating hormonal thinning that would have occurred anyway, just more gradually in a gentler climate.
A study in the Journal of Cosmetic Dermatology examined hair quality in women living in high-hardness water regions versus soft water regions and found that hard water exposure increased hair breakage by 23% in premenopausal women and 41% in perimenopausal women. The hormonally thinned hair simply couldn’t withstand the additional stress.
This doesn’t mean you need to leave the region to preserve your hair. It means you need to be more strategic about protection. Chelating treatments, protective styling that minimizes friction, and products formulated for damaged hair become essential rather than optional. Your body’s adaptation to a new climate takes time, and during perimenopause, that adaptation is happening while your hair’s resilience is already compromised.
What You Can Control (And What You Can’t)
You can’t stop perimenopause. You can’t prevent the hormonal shifts that trigger follicular miniaturization. But you can control how much additional stress you place on already-vulnerable hair, and that makes a measurable difference in how severe the thinning appears.
Minimize heat styling. Hormonally thinned hair has less structural integrity and is more susceptible to heat damage. If you must use heat tools, keep temperatures below 300°F and always use a heat protectant. Better yet, embrace air-drying and low-manipulation styles that reduce mechanical stress.
Address nutritional deficiencies aggressively. A targeted supplement regimen that includes iron (if deficient), vitamin D, omega-3s, and a B-complex can support hair health during the transition. Work with a healthcare provider to identify and correct specific deficiencies rather than taking a scattershot approach.
Manage the environmental factors you can influence. Use a chelating shampoo weekly if you’re in a hard water area. Protect your hair from sun exposure (UV damage compounds structural weakness). Keep your scalp healthy with regular gentle exfoliation to prevent follicular blockage that can worsen thinning. Scalp health becomes even more critical when follicles are already under hormonal stress.
References
- Estrogen and Hair Growth: Mechanism of Action in Female Pattern Hair Loss - Journal of Investigative Dermatology
- Hair Loss as an Early Indicator of Perimenopause: A Longitudinal Study - Menopause: The Journal of The North American Menopause Society
- Androgen Ratios and Female Pattern Hair Loss in Perimenopause - International Journal of Women’s Dermatology
- Hard Water Exposure and Hair Breakage in Pre- and Perimenopausal Women - Journal of Cosmetic Dermatology
- Minoxidil in the Treatment of Female Pattern Hair Loss - American Academy of Dermatology