
You’ve been losing hair for months. Your doctor says it’s hormonal. Your hairdresser blames stress. Your mother insists it’s the water. And you’re standing in the shower watching more strands circle the drain, wondering who’s actually right.
Here’s what makes this frustrating: they might all be partially correct. But the distinction between hormonal and environmental hair loss isn’t just academic. It determines everything from whether treatment will work to how long you’ll wait for regrowth. Get the diagnosis wrong and you’ll spend years treating the wrong problem.
This article contains affiliate links. See our affiliate disclosure for details.
The confusion is understandable. Both types of hair loss can look similar at first glance. Both can be triggered by life changes. Both leave you with thinner hair and mounting concern. But the mechanisms, timelines, and solutions are fundamentally different. Telogen effluvium, the most common form of environmental hair loss, responds to chelation and environmental correction within months. Androgenetic alopecia, the hormonal pattern, requires long-term pharmaceutical intervention and may never fully reverse.
If you’ve recently moved to a hard water region, the distinction becomes even more critical. What looks like hormonal thinning might be mineral buildup strangling your follicles. Or it could be both conditions layered on top of each other, each requiring its own targeted approach.
Pattern vs Distribution: The First Visual Clue
Hormonal hair loss follows a pattern. That’s not metaphorical. Androgenetic alopecia, driven by sensitivity to dihydrotestosterone (DHT), targets specific areas of the scalp in a predictable sequence. In women, this typically means widening of the central part, thinning at the crown, and preservation of the frontal hairline. The Ludwig scale, used by dermatologists to stage female pattern hair loss, documents this progression from subtle part widening to visible scalp exposure along the top of the head.
Environmental hair loss doesn’t respect boundaries. Telogen effluvium, triggered by physical or emotional stress, nutritional deficiency, medication changes, or environmental factors like hard water mineral exposure, causes diffuse shedding across the entire scalp. You’ll lose density everywhere, not just at the crown. The back and sides thin along with the top. Your ponytail gets thinner. Your part gets wider, but so does everything else.
Look at your shedding pattern. If you’re finding short, fine hairs along your hairline and temples, that’s miniaturization, a hallmark of androgenetic alopecia. If you’re shedding full-length hairs with white bulbs attached from all over your head, that’s telogen effluvium. The distinction matters because miniaturized hairs indicate follicle damage from hormonal sensitivity, while full-length shedding indicates a changeed growth cycle that can reset once the trigger is removed.
The timeline of hair loss progression also differs dramatically. Pattern hair loss develops slowly over years, often so gradually you don’t notice until significant density is lost. Environmental hair loss hits fast, usually within two to four months of the triggering event. If your hair was fine six months ago and is noticeably thinner now, environmental factors are more likely than hormones.
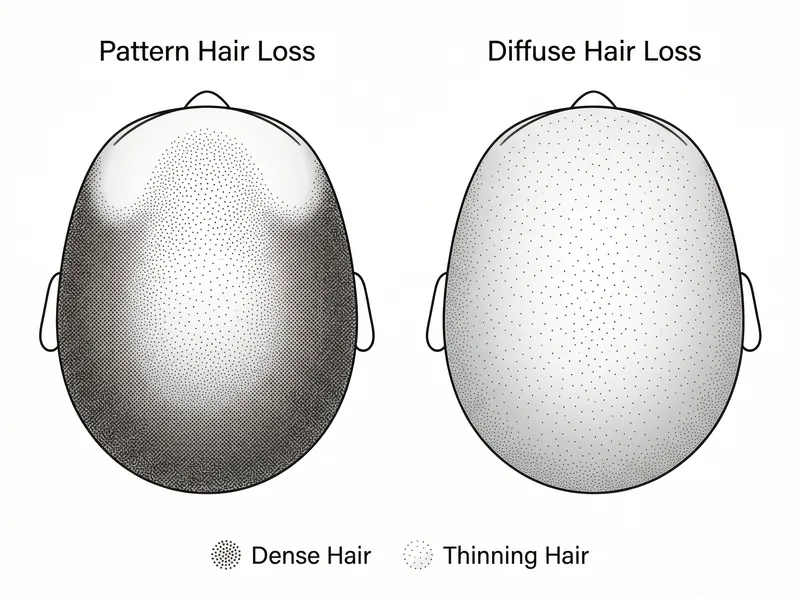 Pattern hair loss (left) shows concentrated thinning at the crown and temples, while diffuse hair loss (right) affects the entire scalp evenly.
Pattern hair loss (left) shows concentrated thinning at the crown and temples, while diffuse hair loss (right) affects the entire scalp evenly.
The Trigger Timeline: When Did This Start?
Hormonal hair loss rarely has a clear starting point. Women with androgenetic alopecia often can’t pinpoint when thinning began. It’s a slow fade, not a sudden shift. You might notice it’s harder to cover your part, or your stylist mentions your hair feels finer, but there’s no obvious ‘before’ moment. This gradual onset reflects the cumulative effect of DHT on genetically susceptible follicles over time.
Environmental hair loss has a trigger you can usually identify. A move to a new city. A period of extreme stress. A crash diet. Postpartum recovery. Research on telogen effluvium shows the shedding phase typically begins 2-4 months after the triggering event, which is the length of the telogen (resting) phase of the hair growth cycle. Your follicles respond to the stressor by prematurely shifting hairs into the shedding phase.
For expats in hard water regions, the trigger is often the environmental transition itself. The first year in a new climate combines multiple stressors: hard water exposure, heat stress, dietary changes, changeed sleep, and psychological adjustment. These compound to push a significant percentage of follicles into telogen simultaneously, resulting in noticeable shedding 8-12 weeks after arrival.
Ask yourself: can I connect my hair loss to a specific life event or change? If yes, environmental factors are likely primary. If no, and the thinning has been gradual and progressive for years, hormonal causes move higher on the differential diagnosis list.
 Environmental hair loss typically shows rapid onset within weeks to months of trigger exposure, while hormonal hair loss develops gradually over years.
Environmental hair loss typically shows rapid onset within weeks to months of trigger exposure, while hormonal hair loss develops gradually over years.
Scalp Health: What Your Roots Are Telling You
Hormonal hair loss doesn’t typically affect scalp health. Your scalp remains normal, without inflammation, flaking, or discomfort. The follicles are shrinking due to hormonal influence, but the surrounding tissue stays healthy. You might notice the hairs themselves are finer and shorter, but your scalp doesn’t hurt, itch, or produce excess oil in response to the thinning.
Environmental hair loss often comes with scalp symptoms. Hard water mineral buildup creates a physical barrier on the scalp surface, leading to itching, flaking, and a tight, uncomfortable sensation. The minerals also change the skin barrier function, potentially triggering inflammation. If your scalp feels different, looks different, or behaves differently since your hair started thinning, environmental factors are implicated.
Examine your scalp closely. Is there visible buildup, whitish residue, or areas of flaking that don’t respond to regular shampooing? Do you have follicular keratosis (small bumps around hair follicles)? Is your scalp producing more oil than usual, or conversely, feeling unusually dry and tight? These symptoms point to external factors affecting scalp health, not internal hormonal shifts.
A simple test: use a chelating shampoo like Regrowth+ designed to remove mineral buildup, and assess whether your scalp feels different within a week. If the tightness, itching, or flaking improves, environmental factors were contributing to your symptoms. This doesn’t rule out concurrent hormonal issues, but it confirms the environment is playing a role.
Family History and Genetic Markers
Hormonal hair loss runs in families. If your mother, grandmother, or sisters experienced progressive hair thinning, your risk of androgenetic alopecia increases significantly. Genetic studies have identified multiple susceptibility genes associated with pattern hair loss, including variants in the androgen receptor gene on the X chromosome, which is inherited from the maternal side.
Environmental hair loss doesn’t care about your genetics. Telogen effluvium is a reactive condition triggered by external stressors. Your family history won’t predict your risk. What matters is your exposure to triggering factors: nutritional deficiencies, physical stress, environmental toxins, or sudden hormonal shifts unrelated to androgenetic patterns.
That said, genetics can influence how your hair responds to environmental stress. Some people’s follicles are more sensitive to mineral buildup or nutritional deficiency. Some recover faster from telogen effluvium than others. But these are response variations, not the inherited progressive miniaturization pattern seen in androgenetic alopecia.
Review your family history honestly. Do the women in your family have progressively thinner hair as they age, particularly with the characteristic widening part and crown thinning? Or do they have full density that occasionally sheds in response to life stressors but generally recovers? The pattern in your family provides clues about your own hair loss mechanism.
Response to Treatment: The Diagnostic Test
Hormonal hair loss responds to anti-androgen treatments. Minoxidil, spironolactone, finasteride (off-label for women), and other DHT-blocking interventions can slow progression and sometimes stimulate regrowth in androgenetic alopecia. But response is gradual, taking 6-12 months to see improvement, and treatment must continue indefinitely. Stop the medication and the thinning resumes.
Environmental hair loss responds to removing the trigger. Address the hard water exposure, correct the nutritional deficiency, manage the stress, or wait out the postpartum recovery period, and shedding stops. Regrowth begins within 3-6 months as follicles re-enter the anagen (growth) phase. No ongoing pharmaceutical intervention is required once the environmental factor is resolved.
This difference makes treatment response a powerful diagnostic tool. If you’ve been using minoxidil for six months with no improvement, but your hair loss started suddenly after a specific trigger, you’re likely treating hormonal hair loss when the actual cause is environmental. Conversely, if chelating shampoos and targeted supplementation haven’t slowed your shedding after three months, hormonal factors may be primary.
Many women have both conditions simultaneously. You might have underlying androgenetic alopecia that was stable and unnoticeable until an environmental stressor triggered acute telogen effluvium, suddenly making the baseline hormonal thinning visible. In these cases, you need to address both the acute trigger and the chronic hormonal component for full recovery.
Diagnostic Testing: What Actually Helps
Hormonal hair loss can be confirmed with specific blood tests and clinical examination. Dermatologists typically check serum ferritin (iron stores), thyroid function, and androgen levels including total testosterone, free testosterone, and DHEA-S. They’ll also perform a clinical scalp examination looking for miniaturization patterns and may use dermoscopy to visualize follicle diameter variation. A scalp biopsy, though rarely needed, can definitively diagnose androgenetic alopecia by showing increased telogen hairs and follicular miniaturization.
Environmental hair loss diagnosis is largely clinical and historical. There’s no blood test for hard water exposure or stress-induced telogen effluvium. Your doctor will take a detailed history looking for triggering events 2-4 months before shedding onset. They’ll examine the shed hairs themselves, looking for telogen bulbs and full-length shafts rather than miniaturized hairs. A pull test, where the doctor gently tugs sections of hair, can reveal increased shedding across all scalp areas in telogen effluvium versus localized shedding in pattern loss.
Don’t skip the blood work even if environmental factors seem obvious. Iron deficiency, thyroid dysfunction, and other systemic issues can trigger or worsen environmental hair loss. You need baseline levels to track whether supplementation or treatment is working. Request a complete panel including ferritin (aim for >70 ng/mL for optimal hair growth), TSH, free T3, free T4, vitamin D, vitamin B12, and zinc.
Water quality testing can provide objective data if you suspect hard water is contributing. Home test kits or professional water analysis will quantify mineral content, particularly calcium and magnesium levels. Readings above 180 mg/L (10.5 grains per gallon) are considered very hard water and likely to cause buildup on hair and scalp over time.
The Gulf Region Context: Why Location Matters
Women in the Gulf region face a unique diagnostic challenge. The environmental factors here are extreme: exceptionally hard desalinated water with high mineral content, intense heat and UV exposure, low humidity, and the compounded stress of expat life. These create a perfect storm for environmental hair loss that can easily be misdiagnosed as hormonal thinning.
Hard water in Gulf countries contains calcium and magnesium concentrations often exceeding 300 mg/L, far above the threshold for hair damage. The minerals bind to hair proteins, creating a coating that prevents moisture absorption, increases friction between strands, and can physically block follicle openings. Over months, this buildup contributes to breakage, dryness, and potentially follicle miniaturization that mimics androgenetic alopecia patterns.
The heat and low humidity add another layer. Temperatures regularly exceeding 40°C (104°F) increase insensible water loss through the scalp, potentially affecting follicle function. UV exposure, particularly intense in this latitude, generates oxidative stress in follicle cells. Combined with the physiological stress of heat adaptation, these factors can trigger widespread telogen effluvium in new arrivals.
If you’ve lived in the Gulf region for less than two years and are experiencing hair loss, environmental factors should be ruled out before assuming hormonal causes. Even if you have a family history of pattern hair loss, the environmental stressors here can unmask or accelerate underlying genetic predisposition. Address the environmental components first, then reassess.
References
- Hard Water and Hair: An Overlooked Environmental Factor - International Journal of Trichology
- Telogen Effluvium: A Complete Review - PubMed Central
- Genetic Variants Associated with Androgenetic Alopecia - PubMed Central
- Female Pattern Hair Loss: Diagnosis and Treatment - American Academy of Dermatology
- Water Quality and Human Health - World Health Organization