
If your lashes look thinner than they used to, you’re not imagining it. And you’re not alone. Women in the Gulf report lash thinning at rates that mirror the scalp hair loss patterns we see here, and the causes overlap more than you’d think.
Eyelashes are hair. They grow from follicles, they cycle through growth phases, and they respond to the same nutritional deficiencies and environmental stressors that affect the hair on your head. The difference? Lash follicles are smaller, more delicate, and they cycle faster. That means problems show up sooner.
This article contains affiliate links. See our affiliate disclosure for details.
The Gulf climate hits lashes hard. Hard water deposits cling to the lash line during daily face washing. UV exposure degrades the keratin structure. Low humidity dries out the follicle environment. And the same iron deficiency causing your scalp hair loss is starving your lash follicles too. Here’s what’s actually happening and what you can do about it.
Why Eyelash Loss Happens: The Biology You Need to Know
Eyelashes grow in a three-phase cycle: anagen (active growth), catagen (transition), and telogen (resting before shedding). Unlike scalp hair, which has an anagen phase lasting years, lash growth only lasts 30 to 45 days. The entire cycle completes in about four to five months.
That short cycle means lashes are constantly turning over. You naturally shed one to five lashes per day. But when something changes the cycle, you notice it fast. If more follicles enter telogen early or stay there too long, you get visible thinning.
Madarosis is the medical term for lash loss. It can be partial (thinning) or complete (total loss). In Gulf residents, we see mostly partial madarosis driven by environmental and nutritional factors, not disease. The follicles aren’t dead. They’re stressed.
A 2017 study in the Journal of Cosmetic Dermatology found that chronic low-grade inflammation around the follicle, often from environmental irritants, shortens the anagen phase and accelerates shedding. That’s exactly what hard water and UV exposure do.
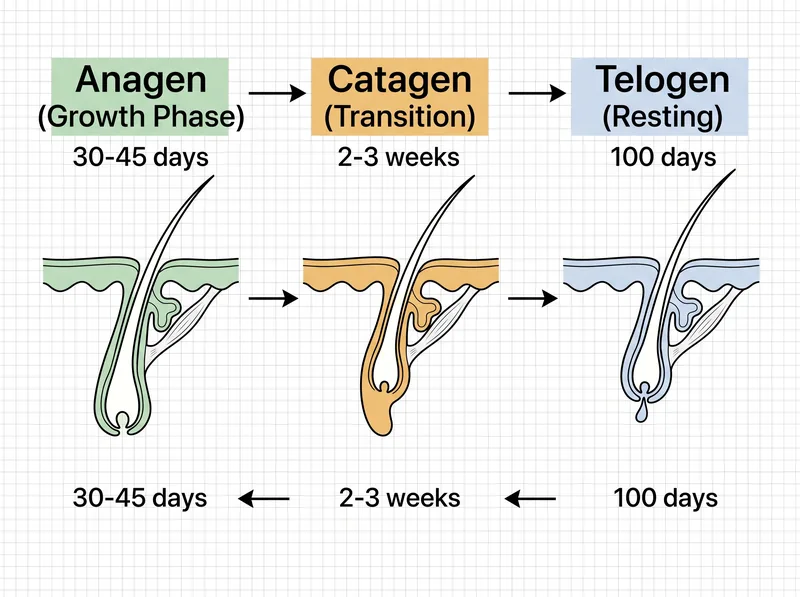 The eyelash growth cycle is shorter than scalp hair, making nutritional deficiencies show up faster.
The eyelash growth cycle is shorter than scalp hair, making nutritional deficiencies show up faster.
Environmental Causes: Hard Water, Heat, and UV Damage
Hard water doesn’t just affect your scalp. Every time you wash your face, mineral deposits coat your lash line. Calcium and magnesium buildup creates a film that clogs the tiny follicle openings and traps debris.
Over time, this buildup causes low-grade folliculitis, microscopic inflammation that weakens the follicle and shortens the growth phase. You won’t see redness or swelling. But you’ll see fewer lashes.
UV exposure is the other environmental factor no one talks about. Eyelashes don’t have the protective pigment density of scalp hair. UVA and UVB rays break down keratin bonds, making lashes brittle and prone to breakage before they complete their natural cycle. Research published in Photochemistry and Photobiology shows that cumulative UV damage to hair shafts reduces tensile strength by up to 30%.
Heat compounds the problem. Ambient temperatures above 40 degrees Celsius dry out the follicle microenvironment, reducing sebum production and leaving lashes without their natural protective coating. It’s the same dryness mechanism affecting your scalp health, just on a smaller scale.
Nutritional Deficiencies: Iron, Biotin, and Protein Gaps
Iron deficiency is the most common nutritional cause of lash thinning in Gulf women. Ferritin below 40 ng/mL changes the anagen phase across all hair follicles, including lashes. You can’t selectively starve one type of hair.
Biotin deficiency is rarer but real. While most women get enough biotin from diet, chronic stress and certain medications (particularly anticonvulsants and antibiotics) deplete it. Biotin is required for keratin synthesis. Without it, lashes grow slower and thinner.
Protein intake matters more than most women realize. Lashes are 97% keratin, a structural protein. If you’re undereating protein (common during Ramadan fasting or postpartum), your body prioritizes vital functions over hair growth. Lashes get deprioritized.
Zinc and vitamin D deficiencies also contribute. A 2019 study in Dermatology and Therapy found that women with madarosis had significantly lower serum zinc and vitamin D levels compared to controls. Both nutrients are critical for follicle health and immune regulation around the follicle.
 Lash loss often starts gradually. By the time you notice gaps, follicle health has already declined.
Lash loss often starts gradually. By the time you notice gaps, follicle health has already declined.
Cosmetic Damage: Mascara, Extensions, and Mechanical Stress
Waterproof mascara is one of the worst offenders. It requires aggressive removal, and the solvents in makeup removers strip the natural oils from lashes. Over time, this makes them dry and brittle. They snap off before completing their growth cycle.
Lash extensions cause traction alopecia of the lash line. The weight of the extension pulls on the natural lash, and the adhesive blocks the follicle opening. When you remove extensions, you often remove the natural lash too, sometimes with the follicle root attached.
Even eyelash curlers cause damage if used daily. The mechanical crimping weakens the lash shaft at the bend point. Curling damp lashes is even worse because wet keratin is more elastic and prone to permanent deformation.
If you’ve been using extensions or waterproof mascara for years and now notice thinning, give your lashes a break. Three months of minimal cosmetics allows the follicles to recover and complete a full growth cycle without interference.
Medical Causes: When Lash Loss Signals Something Bigger
Thyroid disorders cause lash thinning alongside scalp hair loss. Both hypothyroidism and hyperthyroidism change the hair growth cycle, pushing more follicles into telogen. If your lashes are thinning and you’re also experiencing fatigue, weight changes, or temperature sensitivity, get your thyroid checked.
Blepharitis, chronic inflammation of the eyelid margin, causes lash loss through direct follicle damage. You’ll usually notice redness, flaking, or crusting along the lash line. It’s common in Gulf climates because low humidity and hard water both worsen lid inflammation.
Alopecia areata can affect lashes, though it’s less common than scalp involvement. You’ll see patchy lash loss, often asymmetric, with smooth skin where lashes used to be. This is an autoimmune condition requiring dermatological treatment.
Trichotillomania, compulsive lash pulling, is underdiagnosed in women. It often starts as a stress response and becomes habitual. If you find yourself pulling or rubbing your lashes when anxious, especially while working or before sleep, talk to a healthcare provider. It’s treatable.
What Actually Works: Evidence-Based Lash Care
Start with the basics: remove all eye makeup gently every night. Use an oil-based cleanser (micellar water isn’t enough for waterproof formulas) and avoid rubbing. Pat dry, don’t pull.
Address hard water buildup. Use a chelating cleanser once a week on your lash line. The same logic that applies to mineral buildup on scalp hair applies here. A chelating shampoo like Regrowth+ can be used diluted on a clean spoolie brush to gently cleanse the lash line without irritation.
Lash serums with prostaglandin analogs (like bimatoprost) are the only topical treatments with strong clinical evidence for lash growth. They extend the anagen phase and increase follicle density. But they require consistent use and can cause side effects like darkening of the eyelid skin or iris color changes in some users.
Castor oil is popular but evidence is weak. A few small studies suggest it may improve lash appearance through moisturization, but it doesn’t affect the growth cycle. If you use it, apply sparingly to avoid clogging follicles.
Nutritional Support: What to Eat and Supplement
Get your ferritin tested. If it’s below 40 ng/mL, supplement with iron bisglycinate (gentler on the stomach than ferrous sulfate) and pair it with vitamin C for absorption. Aim for ferritin above 70 ng/mL for optimal hair growth.
Protein intake should be at least 0.8 grams per kilogram of body weight daily, more if you’re active or postpartum. Include complete proteins at every meal: eggs, fish, chicken, legumes, dairy. Lashes can’t grow without the building blocks.
Consider a B-complex supplement if you’re on long-term antibiotics or have chronic stress. Biotin alone isn’t enough; you need the full spectrum of B vitamins for keratin synthesis and cellular energy production.
Omega-3 fatty acids reduce inflammation around the follicle and improve sebum quality. A 2015 study in the Journal of Cosmetic Dermatology found that omega-3 supplementation improved hair density and reduced shedding. The same mechanism applies to lashes. Aim for 1,000 mg combined EPA and DHA daily.
References
- Eyelash Growth: Mechanism and Duration of the Growth Phase - Journal of Cosmetic Dermatology
- Ultraviolet Radiation Damage to Hair: Structural and Biochemical Changes - PubMed Central
- Micronutrient Deficiency in Women with Madarosis: A Case-Control Study - Dermatology and Therapy
- Effect of Omega-3 Supplementation on Hair Density and Diameter - Journal of Cosmetic Dermatology
- Madarosis: A Marker of Many Maladies - American Academy of Dermatology