
You’re breaking out along your jawline again. The same spot, the same angry red bumps that weren’t there last month. Or maybe it’s the eczema that cleared up years ago, now back with a vengeance on your hands and inner elbows. Or you’ve caught yourself pulling at your eyebrows during video calls, a habit you thought you’d stopped.
Here’s what’s happening: your mental state is showing up on your skin. This article contains affiliate links. See our affiliate disclosure for details.
The connection between psychological stress and skin conditions isn’t subtle. Research shows that chronic stress directly triggers inflammatory skin responses, worsens existing conditions like acne and eczema, and in some cases, creates compulsive behaviors that damage hair and skin. For women living in high-stress environments (expat transitions, demanding careers, isolation from support networks), the skin becomes a visible map of internal struggle.
This isn’t about blaming yourself for your skin. It’s about understanding the biological mechanisms at play and what actually helps when anxiety is writing itself across your face. Medically reviewed by Dr. Layla Hassan, Trichologist.
Key Takeaways
• Stress triggers a measurable inflammatory cascade in skin through cortisol and neuropeptide release, worsening acne, eczema, and barrier function
• Stress acne appears differently than hormonal acne: clusters on jawline, cheeks, and forehead rather than lower face only
• Trichotillomania (compulsive hair pulling) is an anxiety-related disorder, not a cosmetic habit, and requires psychological intervention alongside hair care
• Environmental stressors (hard water, heat, isolation) compound mental stress, creating a dual assault on skin barrier integrity
• Recovery requires addressing both the stressor and the skin: therapy or stress management plus targeted barrier repair and anti-inflammatory skincare
 The stress-skin axis: how cortisol and inflammation create visible skin changes
The stress-skin axis: how cortisol and inflammation create visible skin changes
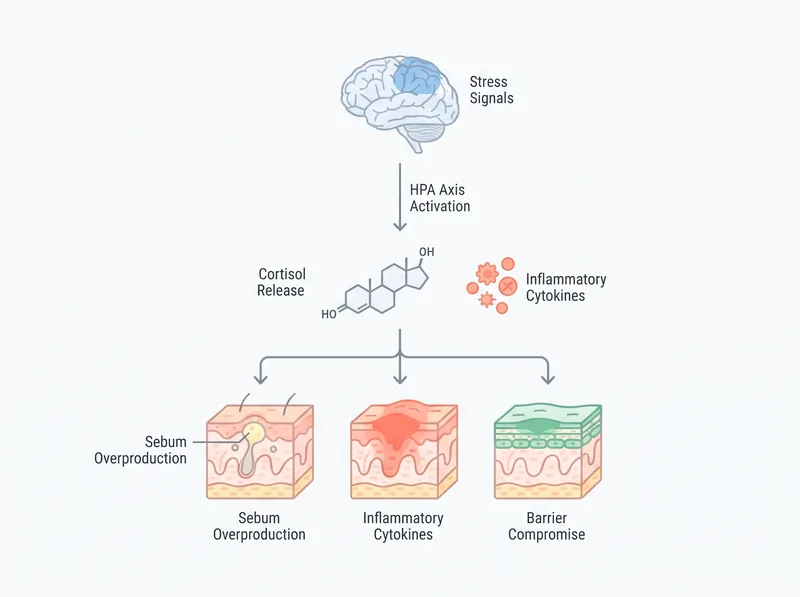
The Stress-Skin Biological Pathway
When you’re stressed, your hypothalamic-pituitary-adrenal axis activates. That’s the system that floods your bloodstream with cortisol. Cortisol does many things, most of them helpful in true emergencies. But chronic improvion creates problems.
In skin, improved cortisol increases sebum production (hello, oily T-zone), suppresses the immune response in ways that allow acne bacteria to thrive, and directly damages the lipid barrier that keeps moisture in and irritants out. Studies show that psychological stress impairs skin barrier recovery by up to 40% compared to non-stressed controls.
There’s also a neuropeptide angle. Skin has its own stress response system, releasing substance P and other inflammatory molecules when you’re anxious. These create the redness, itching, and inflammation you see in stress-triggered eczema flares. Your skin is literally reacting to the same signals your brain is sending.
This isn’t psychosomatic. It’s neuroimmunological. The skin is an organ of the stress response system, not a passive victim of it.
Stress Acne vs Hormonal Acne
They look similar but have different patterns. Hormonal acne (the kind tied to your menstrual cycle) clusters along the lower face and jawline, appearing in the same spots each month. It’s often deeper, cystic, and follows a predictable timeline.
Stress acne is more chaotic. It appears on the forehead, cheeks, and jawline simultaneously. The breakouts are often smaller, more inflamed, and don’t follow your cycle. You might get a cluster after a particularly bad week at work, or during a family crisis, or three months into an expat move when the isolation really hits.
The treatment overlap is significant (barrier repair, anti-inflammatory actives, gentle cleansing), but stress acne won’t fully resolve until you address the stressor. You can’t salicylic-acid your way out of chronic anxiety. You need both the skincare and the stress management.
If you’re in the Gulf and dealing with hard water on top of stress, the barrier damage compounds. The minerals strip your skin’s protective oils, cortisol prevents repair, and you’re stuck in a cycle where everything you apply stings or doesn’t absorb.
 Trichotillomania creates distinctive patterns: missing patches with varying regrowth stages
Trichotillomania creates distinctive patterns: missing patches with varying regrowth stages
Eczema Flares and Anxiety
Eczema (atopic dermatitis) is fundamentally a barrier disorder. The skin can’t hold moisture or keep irritants out. Stress makes this worse through multiple pathways: cortisol thins the skin barrier, inflammatory cytokines increase permeability, and the itch-scratch cycle (which worsens under stress) creates more damage.
Many women report that eczema they had as children returns during periods of high stress. The genetic predisposition was always there, but the environmental trigger (in this case, psychological stress) reactivates it. Research confirms that stress is a primary trigger for eczema flares in adults with a history of atopic disease.
The location matters. Hand eczema is common in women who work in healthcare, food service, or any job requiring frequent handwashing (which strips the barrier). The stress of the job plus the physical barrier assault creates a perfect storm. Eyelid eczema often appears during periods of sleep changeion and anxiety.
Treatment requires aggressive barrier repair (ceramide-rich moisturizers, occlusive layers at night) plus stress reduction. Topical steroids help during acute flares but don’t address the underlying trigger. If you’re dealing with desalinated water that’s already compromising your barrier, the eczema has less margin for error.
Trichotillomania: When Anxiety Targets Hair
Trichotillomania is compulsive hair pulling. It’s not a bad habit. It’s a body-focused repetitive behavior classified under obsessive-compulsive and related disorders. Women pull from the scalp, eyebrows, eyelashes, or pubic area, often without full awareness until the damage is visible.
The pulling provides temporary relief from anxiety or boredom, creating a reinforcement loop. Over time, it becomes automatic. You might pull while reading, watching TV, working at a computer, or lying in bed. The urge builds, the pull releases tension, and the cycle repeats.
What it looks like: irregular bald patches on the scalp, thinned or missing eyebrows (often asymmetrical), sparse eyelashes. The hair in affected areas is at different growth stages because pulling is ongoing. You’ll see very short regrowth, medium stubble, and longer untouched hairs all mixed together. This pattern distinguishes it from other forms of hair loss.
Trichotillomania requires psychological treatment (cognitive behavioral therapy, habit reversal training) as the primary intervention. Skincare and hair care are supportive but won’t stop the behavior. If you’re pulling and also experiencing environmental hair loss from relocation stress, you’re dealing with two separate issues that need different approaches.
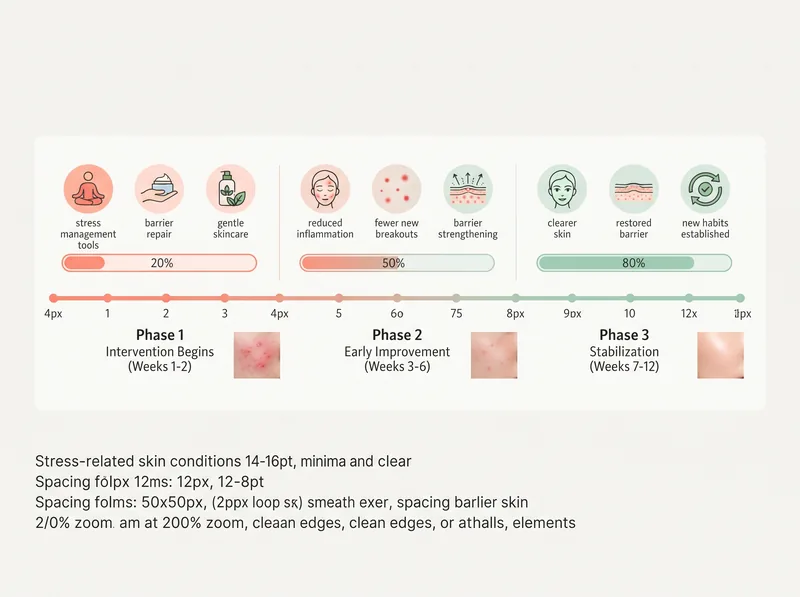 What to expect: stress-skin recovery happens in phases, not overnight
What to expect: stress-skin recovery happens in phases, not overnight
The Expat Stress Multiplier
Expat life creates a specific constellation of stressors: cultural adjustment, language barriers, isolation from family, loss of professional identity, climate shock, and the constant low-grade anxiety of navigating unfamiliar systems. These aren’t acute stressors. They’re chronic, which is worse for skin.
The Gulf environment adds physical stress on top of psychological stress. Hard water damages the barrier. Extreme heat increases inflammation. Indoor AC creates dryness. Dust and pollution trigger immune responses. Your skin is fighting on multiple fronts.
Many women report that their skin was fine for the first few months after moving, then suddenly fell apart around month three or four. That’s when the stress accumulates past the body’s compensation threshold. The initial adrenaline wears off, the reality of long-term adjustment sets in, and the skin shows it.
This is why supporting your body through climate transition requires more than just skincare. You need social connection, routine, purpose, and acknowledgment that what you’re experiencing is hard. The skin will follow the nervous system.
What Actually Helps: The Two-Track Approach
You can’t fix stress skin with skincare alone. You need to address both the stressor and the skin damage. Here’s what works.
Track one: stress reduction. This isn’t about bubble baths and face masks (though those don’t hurt). It’s about identifying your primary stressors and creating containment strategies. Therapy (especially CBT for anxiety or EMDR for trauma) shows measurable cortisol reduction. Regular exercise reduces inflammatory markers. Sleep hygiene (consistent schedule, cool room, no screens) allows barrier repair to happen overnight.
Stress reduction also means saying no. Dropping obligations that don’t serve you. Setting boundaries with people who drain you. Asking for help. These aren’t luxuries. They’re medical interventions for a condition that’s showing up on your face.
Track two: barrier repair and anti-inflammatory skincare. For stress acne, use a gentle cleanser (the hard water in the Gulf already strips your skin, don’t add harsh surfactants), a chelating shampoo like Regrowth+ to remove mineral buildup that clogs pores, niacinamide to reduce inflammation, and a ceramide moisturizer to repair the barrier. For eczema, skip actives during flares and focus on occlusive repair (Vaseline over moisturizer at night works).
When to See a Professional
Some stress-skin connections need medical intervention. See a dermatologist if your acne is cystic, if eczema covers large body areas or doesn’t respond to OTC treatments, or if you’re developing secondary infections from scratching.
See a mental health professional if you’re experiencing panic attacks, persistent insomnia, intrusive thoughts, or if you’ve noticed compulsive behaviors like hair pulling that you can’t stop on your own. Trichotillomania specifically responds well to habit reversal training with a therapist trained in body-focused repetitive behaviors.
If you’re an expat dealing with adjustment disorder (a clinical diagnosis for stress related to major life changes), therapy can prevent the progression to more serious anxiety or depression. Many women wait until they’re in crisis. Early intervention is more effective.
The skin is often the first place stress becomes visible. Don’t ignore what it’s telling you.
References
- The Impact of Psychological Stress on Acne - PubMed Central
- Psychological Stress and Skin Barrier Function - PubMed
- Stress and Atopic Dermatitis - PubMed Central
- Trichotillomania: Clinical Characteristics and Treatment - American Academy of Dermatology
- Neuroendocrine Regulation of Skin Homeostasis - ScienceDirect